
Considerations
If the patient is experiencing acute toxic effects of stimulant use, see Acute Stimulant Intoxication (Overamping).
Screen for suicidality, which may be increased in patients experiencing stimulant intoxication or withdrawal.
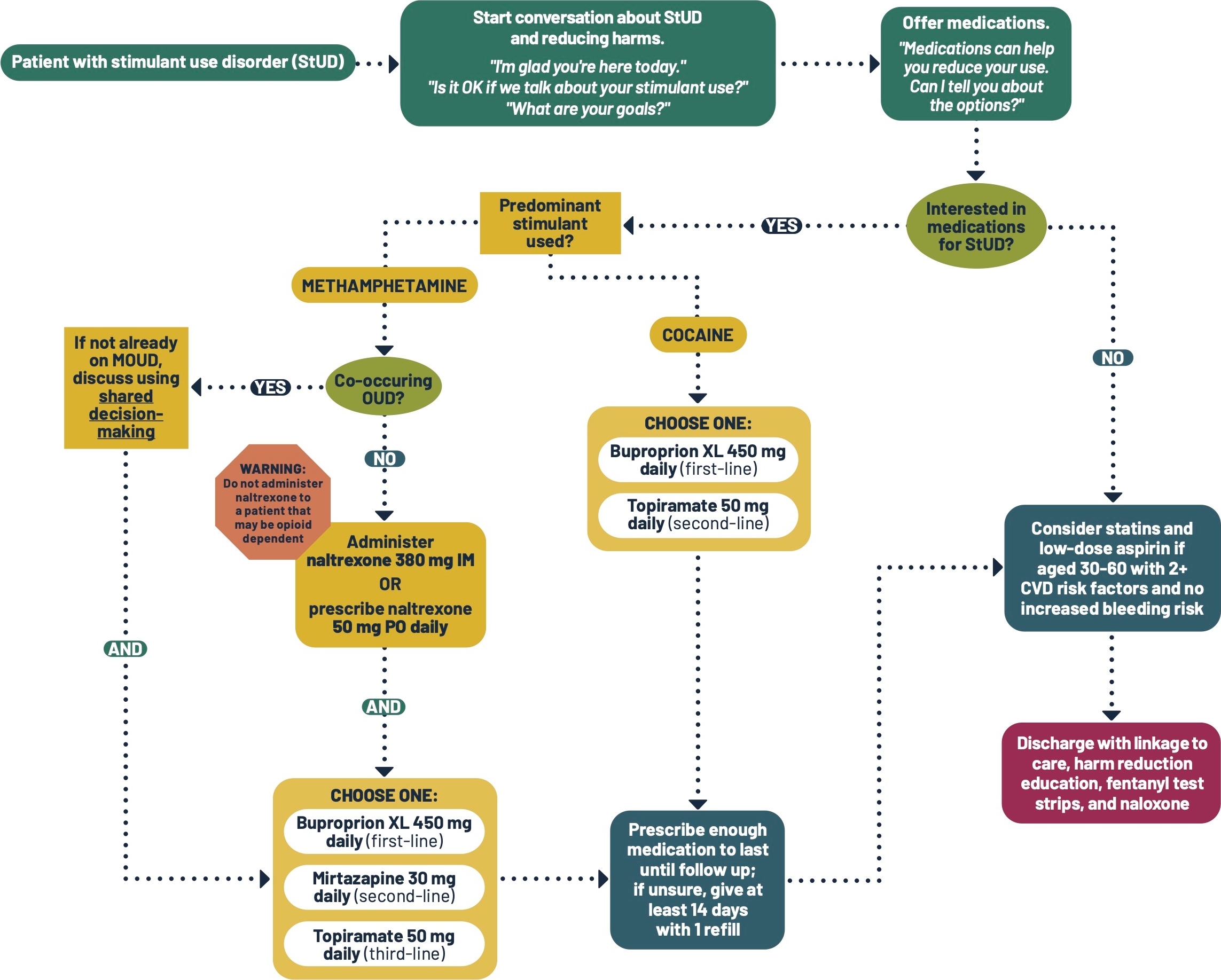
Medications for stimulant use disorder (StUD) are used off label with low to moderate efficacy. Review the Pharmacotherapy section to assist with medication selection. Use shared decision making.
Naltrexone may precipitate delayed, protracted, and severe withdrawal in an opioid-dependent patient. Ask about opioid use and provide education prior to administration.
StUD is associated with increased cardiovascular disease.
Patient Handouts
Additional Clinical Guidance
- Stimulant use disorder (StUD) is treatable.
- Contingency management, in which patients receive small rewards, such as gift cards, for achieving treatment goals, is the most effective intervention, but programs are not widely available.
- Off-label medications can help reduce stimulant use.
- Recovery often requires multiple treatment attempts.
- Stigma prevents help-seeking and worsens health outcomes.
- Care teams must challenge biases to provide compassionate, evidence-based care.
- Use non-stigmatizing, person-first language and trauma-informed care to promote engagement.
- People who use unregulated stimulants are at risk of accidental opioid use and overdose.
- Provide naloxone and fentanyl test strips.
- Use of naltrexone for StUD, when appropriate, has protective benefit.
Assessment
- Assess for withdrawal syndromes.
- Acute stimulant withdrawal:
- Begins within 24 hours of last use.
- Symptoms include depression, anhedonia, hypersomnia, irritability, poor concentration, discomfort or pain, hyperphagia, cravings to use stimulants, and psychomotor agitation or retardation.
- Treatment is supportive care, including being allowed to rest.
- Hypersomnia is common during stimulant withdrawal and should not be confused with sedation resulting from medications for opioid use disorder (MOUD), if administered. If the respiratory rate is adequate, the dose of MOUD is not too high.
- See Acute Stimulant Withdrawal for more information. Assess for other withdrawal syndromes (e.g., opioid, alcohol, benzodiazepines) and treat accordingly. Withdrawal syndromes should be managed swiftly to prevent worsening symptoms and self-directed discharge.
- Acute stimulant withdrawal:
- Assess for opioid dependence and opioid use disorder (OUD) prior to initiating naltrexone.
- Assess for other substance use disorders and treat accordingly.
- Consider screening for mental health comorbidities and referring to psychiatry as appropriate.
- Consider screening for STIs, HIV, and viral hepatitis. People who use stimulants may engage in high-risk sexual behavior.
Labs
- Drug testing is not necessary to initiate treatment of StUD.
- If drug testing is performed for clinical reasons, obtain informed consent.
Pharmacotherapy
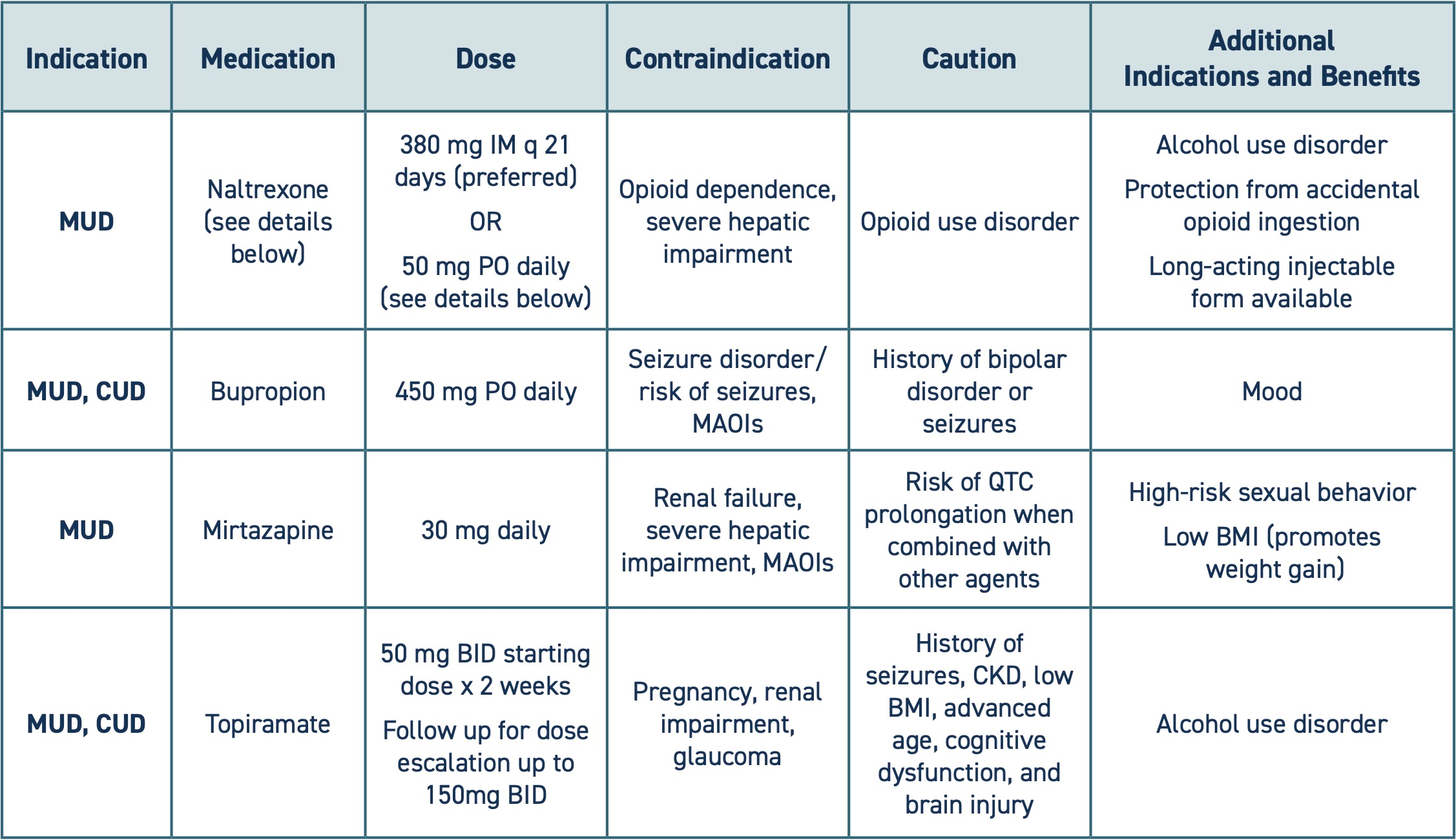
Two forms of StUD, cocaine use disorder (CUD) and methamphetamine use disorder (MUD), are treated differently. Use the following table to aid in shared decision-making.
- Naltrexone:
- Do not administer naltrexone to an opioid-dependent patient. Naltrexone is an opioid antagonist that can precipitate delayed, long-lasting, and severe withdrawal symptoms in an opioid-dependent patient.
- If dependency status is uncertain, consider a test dose of naloxone 0.4 mg, as it is shorter acting. Reassure the patient that if withdrawal occurs, symptoms will be treated. See Opioid Withdrawal in Acute Care Settings.
- If withdrawal was induced, offer MOUD (return to "co-occurring OUD" in algorithm).
- Co-occurring opioid use disorder (OUD):
- Patients who have primary StUD and secondary OUD may not identify as having OUD and be hesitant to accept MOUD. Discuss the benefits, including significant reduction of opioid overdose risk and death, and prevention of withdrawal.
- Buprenorphine and methadone are the preferred treatments and cannot be combined with naltrexone.
- Naltrexone is a second-line option for OUD. It may be suitable to treat co-occurring OUD and StUD in some patients, such as in cases of prolonged abstinence from opioids, and with careful education regarding high overdose risk at treatment cessation.
- Offer long-acting injectable naltrexone (Vivitrol) for consistent plasma levels.
- Do not administer naltrexone to an opioid-dependent patient. Naltrexone is an opioid antagonist that can precipitate delayed, long-lasting, and severe withdrawal symptoms in an opioid-dependent patient.
- Extended-release stimulants (e.g., amphetamine/dextroamphetamine) may be appropriate in the context of co-occurring ADHD. Refer to addiction medicine or psychiatry.
- Low-dose aspirin and/or statins may lower the risks of cardiovascular disease associated with StUD. Consider starting statins and low-dose aspirin for those aged 30-60 with 2 or more risk factors for CVD (HTN, high cholesterol, DM, smoker) and no increased bleeding risk.
Pathophysiology
- High-potency stimulants like cocaine and methamphetamine can be acutely and chronically vascular and neuro-toxic.
- Chronically elevated dopamine levels trigger neuroinflammation and cell death, contributing to neurodegeneration and psychosis.
- Vasoconstriction and inflammation induced by stimulants can contribute to vascular disease, including hypertension, dilated cardiomyopathy, heart failure, atherosclerosis, arrythmias, aortic dissection, cerebrovascular disease, pulmonary and renovascular hypertension, and intestinal ischemia.
- STI and blood borne pathogen risk:
- Stimulant use may increase sex drive and impulsivity and reduce inhibitions, increasing the likelihood of engaging in risky sexual practices.
- Methamphetamine use is associated with higher rates of HIV and viral hepatitis.
Special populations
- Pregnancy considerations:
- Medications:
- Topiramate is contraindicated in pregnancy.
- Naltrexone can be used safely during pregnancy, although data is limited.
- Bupropion and mirtazapine can be used in pregnancy, although there are associated risks. Weigh the risks and benefits prior to initiating treatment.
- Prenatal care is important. A non-judgmental, trauma-informed approach may encourage engagement with prenatal care.
- In Washington state, parental drug use alone does not require a Child Protective Services (CPS) referral.
- Medications:
Polysubstance use
- Ask about other substance use and educate on strategies to reduce harm and offer treatment options.
Administration
- Naltrexone:
- If naltrexone is appropriate and it is unfeasible to initiate LAI naltrexone (Vivitrol), it is reasonable to prescribe the oral formulation while linking to an outpatient provider that can administer the injection.
Discharge planning
- Help the patient schedule a follow-up appointment with primary care and/or offer information on available walk-in clinics, when available, to reduce barriers to care.
- StUD medication management may be done by primary care, psychiatry, or a substance use disorder treatment program that has a prescriber.
- Primary care is also important for management of correlated health issues, including cardiac and sexual health risk factors.
- Offer a referral to a behavioral-based StUD treatment program.
- Contingency management has demonstrated the highest efficacy for StUD treatment. Contingency management programs provide participants with small rewards for achieving treatment goals. See the Health Care Authority’s Contingency Management factsheet for program locations.
- Cognitive Behavioral Therapy, Community Reinforcement Approach, and the Matrix Model are also evidence-based therapies. Outpatient or residential treatment programs can be found in the Department of Health’s Behavioral Health Agency Greenbook.
- Ensure patients have enough medication to last until they can follow up with a prescriber. At least 7-14 days prescription length is advised.
- Provide the Stimulants and Health handout.
- Provide naloxone, even without known opioid use. People who use unregulated stimulants are at risk for unknowingly consuming opioids.
- In Washington, emergency departments are required to dispense naloxone to patients who are at risk of opioid overdose, in compliance with SB5195. Ensure patients are discharged with naloxone in hand.
- If possible, connect patients with additional support such as social work, care navigation, or peer support to improve patient experience and linkage to care.
Patient education
- Discuss strategies for improving health and reducing the harms of substance use.
- Do this with empathy. Changing behavior can be extremely difficult.
- Use the Stimulants and Health handout and the Guide to Using the Handout for more effective conversations.
- See Discharge Instructions for tips to prevent overamping and overdose.
- Recommend safer sex practices, including condoms and PrEP.
- Educate on strategies to reduce harms related to other substance use, if any.
Discharge Instructions
Medication information
You may have been prescribed medications to help you manage your stimulant use. When taken regularly, these medications can help reduce your cravings to use. You may have been prescribed one or more of these medications:
- Naltrexone 380 mg monthly injectable OR oral naltrexone 50 mg once daily
- Follow up with a health care provider to start (or continue) monthly injectable naltrexone.
- Naltrexone blocks the effects of opioids. If you experience an injury or other severe acute pain that requires opioid medications, tell your care team that you are taking this medication.
- Tell your health care provider if you:
- Have yellowing of the whites of the eyes or very dark urine.
- Have new or worsening depression or suicidal thoughts.
- Bupropion 450 mg once daily
- This medication can make seizures more likely to occur if you:
- Have a seizure disorder.
- Consistently use alcohol heavily and stop abruptly.
- Do not take this medication with monoamine oxidase inhibitors (MAOIs) such as Selegiline (Emsam), Isocarboxazid (Marplan), Tranylcypromine (Parnate), and Phenelzine (Nardil), or within 14 days of stopping an MAOI.
- Tell your health care provider if you have suicidal thoughts or unexpected changes in mood or behavior.
- This medication can make seizures more likely to occur if you:
- Mirtazapine 30 mg once daily
- This medication may make you sleepy.
- You may choose to take it at bedtime.
- Avoid or limit other sedating medications, drugs, or alcohol.
- Be cautious when driving or operating heavy machinery until you know how mirtazapine affects you.
- Do not stop this medication abruptly. It should be tapered down with the help of a provider.
- Tell your health care provider if you have new or worsening symptoms of depression or suicidal thoughts.
- This medication may make you sleepy.
Topiramate 50 mg twice daily x2 weeks, to start
- This medication is started at a low dose and increased over time. Follow up with a provider to increase the dose to get the desired effect.
- Do not stop this medication abruptly. It should be tapered down with the help of a provider.
- If you miss a dose, take it as soon as possible, unless it is within 6 hours of the next dose.
Follow up with a health care provider to continue these medications or make changes to your treatment plan.
Overamping and overdose prevention
Overamping can happen when a person uses too much methamphetamine or cocaine or uses for too long without a break. The biggest risks of overamping include overheating, heart attack, stroke, seizure, severe anxiety/paranoia, and trouble thinking.
Using street drugs is risky. People who use unregulated drugs, like cocaine and methamphetamine, are also at risk of opioid overdose if they accidentally use an opioid like fentanyl.
Reduce your risk of dying from an opioid overdose with the following strategies:
- Call 911 right away if someone:
- Might hurt themselves or someone else.
- Stops responding, passes out, or can’t wake up.
- Has chest pain, numb limbs, splitting headache, slurred or jumbled speech, confusion, or shaking.
- Can’t walk or move.
- Has slow, abnormal, or no breathing.
- Avoid using too much or for too long.
- If you feel close to your limit, don't use more.
- Methamphetamine can stay in your body for a long time.
- Take breaks. Avoid using for multiple days in a row.
- Get enough sleep.
- When you take breaks, make sure to rest and sleep as much as possible.
- Eat and drink.
- Drink plenty of water and eat food before you use and throughout your high.
- Try to eat small amounts even if you do not feel hungry.
- Set an alarm on your phone to remind you to eat and drink.
- Try not to use alone.
- Use where you feel safe and with people who will help you if needed.
- Start low and go slow.
- You can't know the full contents or strength of drugs. If you use, start with a small amount to see how it affects you.
- Be extra cautious if you have low tolerance (for example, after not using for a while). If you decide to use more, slowly increase in small amounts.
- Watch and wait before next person uses.
- If you’re with a group of people, take turns to see how the drug is affecting people. Someone needs to be able to ask for help.
- Avoid mixing drugs.
- Mixing drugs increases the risks. If you do use multiple drugs, try to use one at a time and use less of each.
- Check your drugs.
- Fentanyl test strips can help you avoid fentanyl.
- False positives are common when testing methamphetamine for fentanyl. Make sure to dilute your sample with more water than is needed to test opioids and follow the instructions carefully.
- Drug checking machines provide more information.
- Learn more at a syringe service program.
- Always have naloxone (Narcan).
- Naloxone is a medication that reverses opioid overdose. It is safe to use on anyone you think may be experiencing an overdose.
- Even if you don’t use opioids (like fentanyl), have naloxone ready. Street drugs can be mixed up or contaminated with unexpected substances.
- Tell others you have naloxone, where it is, and when to use it.
- Visit stopoverdose.org or talk to your provider, nurse, or pharmacist to learn more or get more naloxone.
- Consider treatment to reduce or stop use.
- Contingency Management is effective for stimulant use disorder.
- In contingency management programs, patients receive small rewards for achieving treatment goals.
- More information and program locations can be found at https://www.hca.wa.gov/assets/program/fact-sheet-contingency-management.pdf
- Residential and outpatient programs may also be helpful. If you need help finding a treatment provider, call the Washington Recovery Helpline at 866-789-1511 or go to warecoveryhelpline.org.
- Learn more about treatment options at learnabouttreatment.org.
- Contingency Management is effective for stimulant use disorder.
Additional Resources
- HCA Contingency Management factsheet
- Contingency Management Resource Hub
- Behavioral Health Agency Greenbook to find outpatient and inpatient/residential treatment programs.
- Concurrent stimulant and opioid use
- Acute stimulant withdrawal
References
- Atluru S, Bruehlman AK, Vaughn P, Schauberger CW, Smid MC. Naltrexone Compared with Buprenorphine or Methadone in Pregnancy: A Systematic Review. Obstet Gynecol. 2024;143(3):403-410. doi:10.1097/AOG.0000000000005510
- Bureau of Substance Addiction Services (BSAS). Stimulant Use Disorder Treatment. n.d. Retrieved 6/5/2025 from: https://www.mass.gov/doc/stimulant-use-disorder-treatment-guidance-pdf/download
- Center for Innovative Academic Detailing on Opioids and Stimulants at the San Francisco Department of Public Health (CIAO SFDPH). Opioids and Stimulants: A Guide for Healthcare Providers. San Francisco, CA. April 2024
- Clinical Guideline Committee (CGC) Members ; ASAM Team ; AAAP Team ; IRETA Team . The ASAM/AAAP Clinical Practice Guideline on the Management of Stimulant Use Disorder. J Addict Med. 2024;18(1S Suppl 1):1-56. doi:10.1097/ADM.0000000000001299
- Coffin PO, Suen LW. Methamphetamine Toxicities and Clinical Management. NEJM Evid. 2023;2(12):EVIDra2300160. doi:10.1056/EVIDra230016
- Li MJ, Shoptaw SJ. Clinical management of psychostimulant withdrawal: review of the evidence. Addiction. 2023;118(4):750-762. doi:10.1111/add.16093
- Newton TF, Kalechstein AD, Duran S, Vansluis N, Ling W. Am J Addict. 2004;13(3):248.
- Stimulant treatment and recovery team clinical guidelines: a collaborative care approach. 2024. Boston Medical Center. Retrieved 10/6/2025 from: https://addictiontraining.org/documents/resources/409_START_Stimulant_Clinical_Guidelines.pdf

