
Considerations
Overamping refers to acute toxic effects of high doses or extended use of high-potency psychostimulants like methamphetamine and cocaine.
High-potency stimulants can be acutely vascular and neuro-toxic.
Prolonged exposure can accelerate development of chronic cardiovascular and neurologic pathology.
Hyperadrenergic symptoms may include: tachycardia, hypertension, hyperthermia
- The initial blood pressure goal is to lower SBP by no more than 20% from pre-treatment.
Psychiatric symptoms may include: psychosis, paranoia, hallucinations, agitated delirium
- Use de-escalation techniques.
- Monitor for suicidality.
- Evaluate for and address any additional underlying causes of agitation.
- It is difficult to distinguish between stimulant-induced psychosis and primary psychosis. In the acute setting, the treatment is the same. Patients should be referred for ongoing management.
- Consult (e.g., toxicology, cardiology) for complex cases. The WA Poison Center can be reached at 800-222-1222.
Potential complications
- Chest pain: vasodilator (calcium channel blocker, nitroglycerin)
- QRS widening (cocaine-induced): sodium bicarbonate
- Hypertensive emergency:
- Use short-acting agents (nitroprusside, phentolamine, dihydropyridine calcium channel blocker).
- Avoid long-acting agents due to risk of hemodynamic collapse.
- Add nitroglycerin for cardiac ischema.
- Seizure
- First-line: benzodiazepines
- Refractory seizures: phenobarbital or propofol
- Myocardial infarction, hyperthermia/heat stroke, metabolic acidosis, rhabdomyolysis: use existing hospital protocols
Patient Handouts
Additional Clinical Guidance
- It is difficult to distinguish between stimulant-induced psychosis and primary psychosis; in the acute setting, the treatment is the same and includes de-escalation and antipsychotic and sedative medications.
- De-escalate mild to moderate agitation to keep the patient, yourself, and others safe until the patient is stabilized.
- Create a calm and safe environment: quiet, low-light, clear exit.
- Remain calm.
- Maintain physical distance and a non-threatening posture.
- Speak concisely; repeat and allow processing time.
- Identify and acknowledge patient's wants and feelings.
- Offer choices and control (food, water, blankets).
- Provide reassurance of safety, that symptoms will resolve.
- Set clear boundaries when staff safety is threatened.
- Be consistent (e.g., designate one provider to attend to the patient).
- Use restraints only when necessary to prevent harm to self/others.
Assessment
- Assess and monitor for suicidality, which may be increased in patients experiencing stimulant withdrawal or intoxication.
- Once stabilized, assess for stimulant use disorder (StUD) and offer treatment medications. See Related Protocols.
Pharmacotherapy
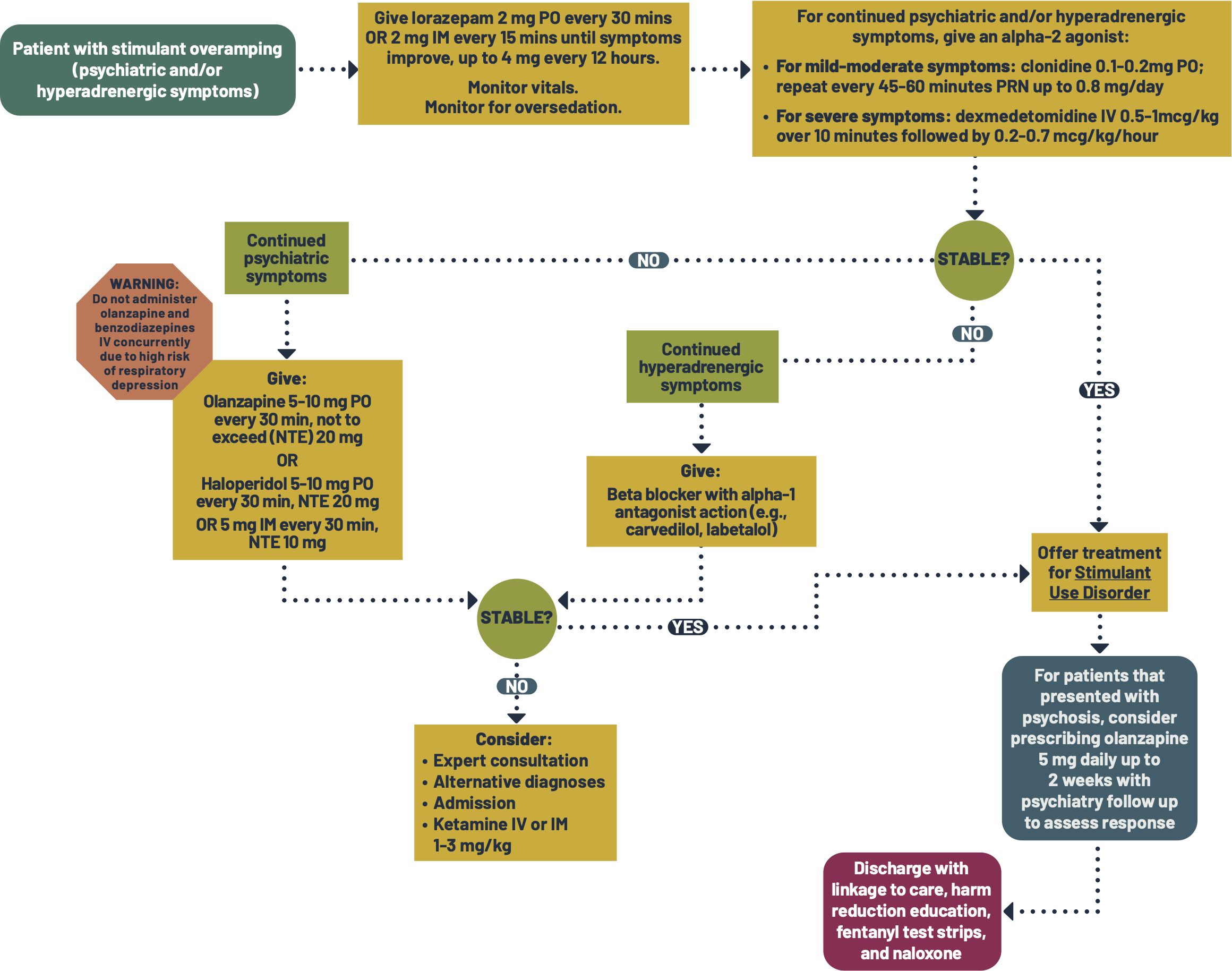
- Primary treatment for stimulant toxicity is GABAergic agents (e.g., benzodiazepines, phenobarbital, propofol). Benzodiazepines are generally considered first-line.
- Benzodiazepines (first-line for overamping):
- Short-acting benzodiazepines, like lorazepam or midazolam, are effective for both psychiatric and hyperadrenergic symptoms of overamping.
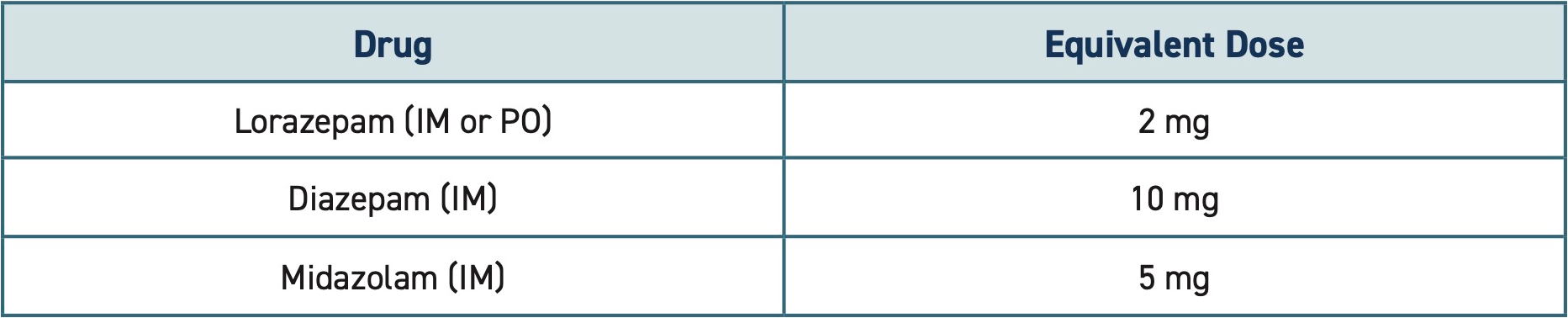
- Short-acting benzodiazepines, like lorazepam or midazolam, are effective for both psychiatric and hyperadrenergic symptoms of overamping.
- Antipsychotics (second-line for psychiatric symptoms):
- Antipsychotics are second-line treatment for psychiatric symptoms and can be used in addition to benzodiazepines.
- Aripiprazole, quetiapine, haloperidol, olanzapine, and risperidone effectively treat both positive and negative symptoms of stimulant-induced/associated psychosis.
- Avoid chlorpromazine and clozapine due to increased seizure risk.
- If presenting with or has a history of psychotic symptoms, consider prescribing olanzapine 5 mg daily for 2 weeks and refer to psychiatry (or any available provider) for follow up.
- Second generation antipsychotics at this dose are safe and have no abuse potential.
- Currently there is little data to support prescribing PRN antipsychotics at discharge for stimulant-induced psychosis, but some practitioners have reported positive outcomes.
Alpha-2 adrenergic agonists (second-line for hyperadrenergic symptoms):
- Alpha-2 adrenergic agonists can be effective in treating stimulant-induced agitation, hypertension, and tachycardia.
- Clonidine is used for mild to moderate symptoms.
- Dexmedetomidine IV may be used for severe symptoms.
- Use of dexmedetomidine varies by institution and is sometimes reserved for the ICU. If available, follow institutional protocols or seek guidance from a pharmacist or intensivist.
- If dexmedetomidine is unavailable, consider clonidine and a beta blocker with alpha-1 antagonist action.
- Beta blockers with alpha-1 antagonist action (third-line for hyperadrenergic symptoms):
- If a beta blocker is used, one with alpha-1 antagonist action (e.g., labetalol carvedilol) is generally preferred.
- This is due to a theoretical risk of unopposed alpha stimulation leading to increased blood pressure and/or coronary artery vasoconstriction.
- If an unopposed beta blocker was already used, consider adding a coronary vasodilator (e.g., nitroglycerin, calcium channel blocker).
- If a beta blocker is used, one with alpha-1 antagonist action (e.g., labetalol carvedilol) is generally preferred.
- Avoid long acting antihypertensives (e.g., lisinopril, losartan, amlodipine, metoprolol) due to risk of hemodynamic collapse in cases of hypertensive emergency.
Pathophysiology
- High-potency stimulants like cocaine and methamphetamine can be acutely and chronically vascular and neuro-toxic.
- Intoxication can result in:
- Behavioral symptoms like confusion, paranoia, irritability, hypersexuality, and hyper vigilance.
- Physiological signs and symptoms can include elevated body temperature, rapid heart rate, elevated blood pressure, chest pain, and neurologic problems.
- Acute toxicity:
- Acute toxic effects of high dose or extended use of high-potency psychostimulants is referred to as overamping.
- Overamping can be life-threatening. Complications include:
- Psychosis, paranoia, hallucinations, agitated delirium
- Cardiovascular events (e.g., ACS, hypertensive emergency, MI)
- Seizure
- Hyperthermia/heat stroke
- Acidosis
- Rhabdomyolysis
- Renal failure
- Treat physiological symptoms per clinical judgement and existing protocols.
Special populations
Pregnancy:
- This protocol can be used in pregnant patients with assessment of risks and benefits. Some medications may pose risks to the fetus, but the risk of untreated overamping may be higher.
Patient safety
Seclusion and physical or chemical restraints may only be used in accordance with federal and Washington state law and institutional policy. Seclusion and restraints must be:
- Used only as a last resort and only after less restrictive measures have failed.
- Limited to the extent and duration necessary to ensure safety.
- As least restrictive as possible.
- Monitored frequently.
- Ordered and periodically reviewed and renewed by a physician, physician assistant, or psychiatric advanced registered nurse practitioner.
Discharge planning
- Help the patient schedule a follow-up appointment with primary care and/or offer information on available walk-in clinics, when available, to reduce barriers to care.
- Provide the Stimulants and Health handout.
- Provide naloxone, even without known opioid use. People who use unregulated stimulants are at risk for unknowingly consuming opioids.
- In Washington, emergency departments are required to dispense naloxone to patients who are at risk of opioid overdose, in compliance with SB5195. Ensure patients are discharged with naloxone in hand.
- If possible, connect patients with additional support such as social work, care navigation, or peer support to improve patient experience and linkage to care.
Patient education
- Discuss strategies for reducing the harms of drug use (see Discharge Instructions).
- This should be done with empathy. Reducing or stopping use is often extremely difficult.
- Recommend safer sex practices, including condoms and PrEP.
- Educate on strategies to reduce harms related to other substance use, if any.
Discharge Instructions
Tips to prevent overamping and overdose if you use drugs
Using street drugs is risky. Overamping can happen when a person uses too much methamphetamine or cocaine or uses for too long without a break. The biggest risks of overamping include overheating, heart attack, stroke, seizure, severe anxiety/paranoia, and trouble thinking. People who use unregulated drugs, like cocaine and methamphetamine, are also at risk of opioid overdose if they accidentally use an opioid like fentanyl. You can reduce your risk of dying from overamping and overdose with the following strategies:
- Call 911 right away if someone:
- Might hurt themselves or someone else.
- Stops responding, passes out, or can’t wake up.
- Has chest pain, numb limbs, splitting headache, slurred or jumbled speech,
confusion, or shaking. - Can’t walk or move.
- Has slow, abnormal, or no breathing.
- Avoid using too much or for too long.
- If you feel close to your limit, don't use more.
- Methamphetamine can stay in your body for a long time.
- Take breaks. Avoid using for multiple days in a row.
- Get enough sleep.
- When you take breaks, make sure to rest and sleep as much as possible.
- Eat and drink.
- Drink plenty of water and eat food before you use and throughout your high.
- Try to eat small amounts even if you do not feel hungry.
- Set an alarm on your phone to remind you to eat and drink.
- Try not to use alone.
- Use where you feel safe and with people who will help you if needed.
- Start low and go slow.
- You can't know the full contents or strength of drugs. If you use, start with a
small amount to see how it affects you. - Be extra cautious if you have low tolerance (for example, after not using for a
while). If you decide to use more, slowly increase in small amounts.
- You can't know the full contents or strength of drugs. If you use, start with a
- Watch and wait before next person uses.
- If you’re with a group of people, take turns to see how the drug is affecting
people. Someone needs to be able to ask for help.
- If you’re with a group of people, take turns to see how the drug is affecting
- Avoid mixing drugs.
- Mixing drugs increases the risks. If you do use multiple drugs, try to use one
at a time and use less of each.
- Mixing drugs increases the risks. If you do use multiple drugs, try to use one
- Check your drugs.
- Fentanyl test strips can help you avoid fentanyl.
- False positives are common when testing methamphetamine for fentanyl.
Make sure to dilute your sample with plenty of water (dilute residue in ½ cup
of water) and follow the instructions carefully. - Drug checking machines provide more information.
- Learn more at a syringe service program.
- Always have naloxone (Narcan).
- Naloxone is a medication that reverses opioid overdose. It is safe to use on
anyone you think may be experiencing an overdose. - Even if you don’t use opioids (like fentanyl), have naloxone ready. Street
drugs can be mixed up or contaminated with unexpected substances. - Tell others you have naloxone, where it is, and when to use it.
- Visit stopoverdose.org or talk to your provider, nurse, or pharmacist to learn
more or get more naloxone.
- Naloxone is a medication that reverses opioid overdose. It is safe to use on
- Consider treatment to reduce or stop use.
- Contingency Management is effective for stimulant use disorder.
- In contingency management programs, patients receive small
rewards, such as gift cards, for achieving treatment goals. - More information and program locations can be found at
https://www.hca.wa.gov/assets/program/fact-sheet-contingency-management.pdf
- In contingency management programs, patients receive small
- Residential and outpatient programs may also be helpful. If you need help
finding a treatment provider, call the Washington Recovery Helpline at 866-
789-1511 or go to warecoveryhelpline.org. - Learn more about treatment options at learnabouttreatment.org.
- Contingency Management is effective for stimulant use disorder.
Additional Resources
- Stopoverdose.org for more info about stimulant overamping.
- Concurrent stimulant and opioid use
References
- Bureau of Substance Addiction Services (BSAS). Stimulant Use Disorder Treatment. n.d. Retrieved 6/5/2025 from: https://www.mass.gov/doc/stimulant-use-disorder-treatment-guidance-pdf/download
- Clinical Guideline Committee (CGC) Members ; ASAM Team ; AAAP Team ; IRETA Team. The ASAM/AAAP Clinical Practice Guideline on the Management of Stimulant Use Disorder. J Addict Med. 2024;18(1S Suppl 1):1-56. doi:10.1097/ADM.0000000000001299
- Coffin PO, Chang YG, McDaniel M, et al. Evaluation of methamphetamine assist packs: As-needed antipsychotics for self-management of methamphetamine-associated psychiatric toxicity. Int J Drug Policy. 2024;129:104480. doi:10.1016/j.drugpo.2024.104480
- Fluyau D, Mitra P, Lorthe K. Antipsychotics for Amphetamine Psychosis. A Systematic Review. Front Psychiatry. 2019 Oct 15;10:740. doi: 10.3389/fpsyt.2019.00740. PMID: 31681046; PMCID: PMC6804571
- Houston MC. Treatment of hypertensive emergencies and urgencies with oral clonidine loading and titration. A review.Arch Intern Med 1986;146(3):586-589.
- Li MJ, Shoptaw SJ. Clinical management of psychostimulant withdrawal: review of the evidence. Addiction. 2023;118(4):750-762. doi:10.1111/add.16093
- Stimulant treatment and recovery team clinical guidelines: a collaborative care approach. 2024. Boston Medical Center. Retrieved 10/6/2025 from: https://addictiontraining.org/documents/resources/409_START_Stimulant_Clinical_Guidelines.pdf

