
Considerations
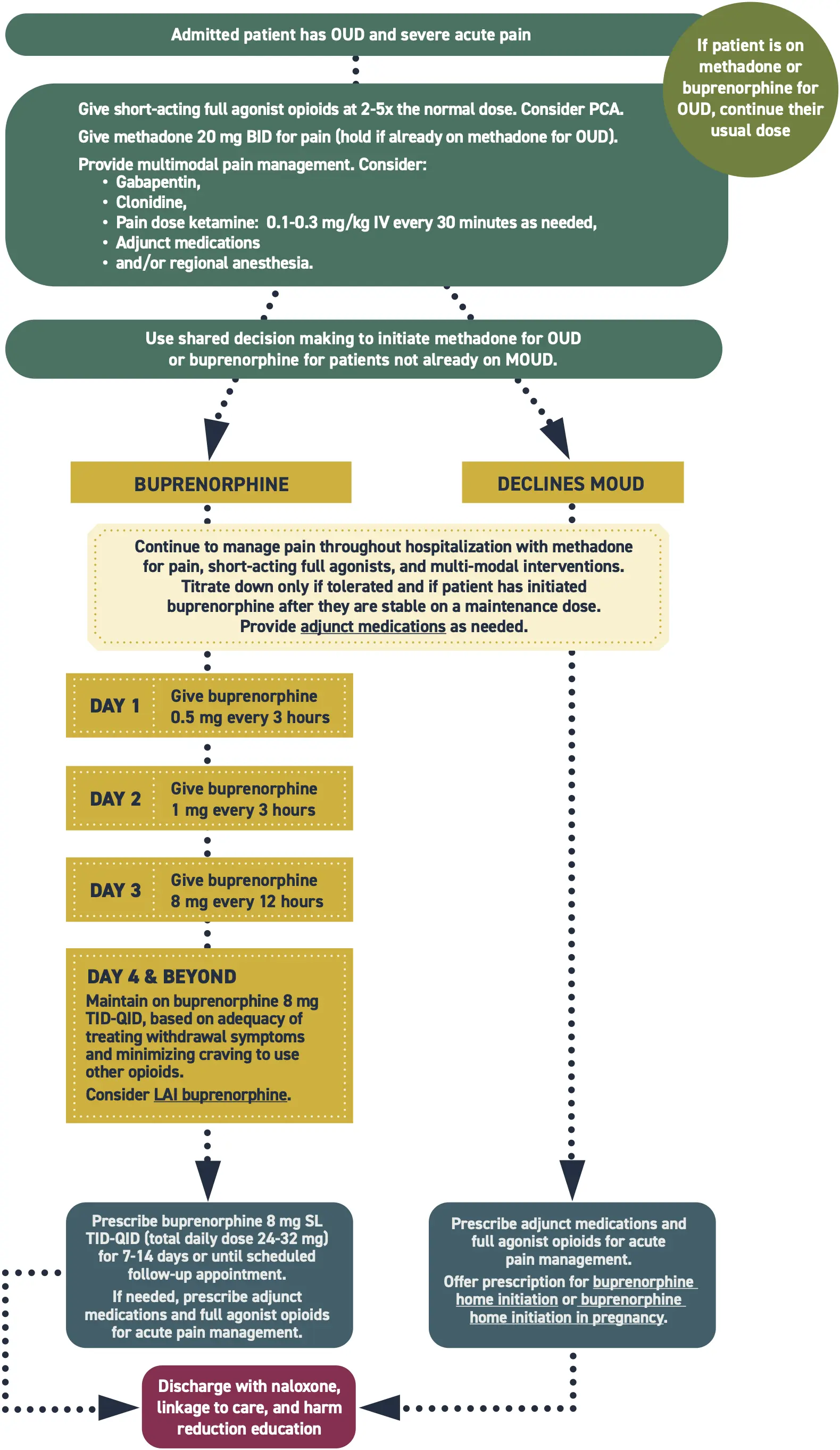
Higher doses of opioids for analgesia are required for patients with opioid tolerance; 2-5x the usual dose is typically needed to adequately control pain.
The risk of respiratory depression in this case is low. If respiratory rate remains within normal limits and the patient is not overly sedated, the dose is not too high.
Ensure pain is adequately controlled and opioid withdrawal is prevented/ managed to prevent self-directed discharge.
Discussion of MOUD treatment options is more effective when pain and withdrawal are well-managed.
Treating acute pain does not worsen OUD.
Full agonist opioids, including methadone, can be used safely to treat acute pain in addition to initiating buprenorphine for OUD.
This protocol can be used for pregnant and postpartum patients. See Special Populations for more information
This protocol does not cover the care of patients on naltrexone. Consider expert consultation.
Additional Clinical Guidance
- Acute pain is treatable and should be managed in patients with opioid use disorder (OUD). Untreated or undertreated pain may prevent patients from completing needed medical care, cause physical and psychological harm, and place patients at high risk for overdose.
- Patients with OUD should have their pain and withdrawal adequately managed regardless of, and prior to deciding, plans to continue OUD treatment after discharge.
- Evidence supports treating both OUD and pain simultaneously. Methadone and buprenorphine should be maintained or can be initiated during an acute pain episode such as post-op, injury, or trauma. Full agonist opioids can be safely used and titrated to relieve pain.
- Patients with OUD are highly stigmatized. Stigma prevents people from seeking care or reaching out for help when they need it. Providers should reflect on and challenge biases to provide compassionate and evidence-based care that improves outcomes.
Assessment
- Ask the patient about the type, amount, and frequency of opioids they are currently taking. This can help gauge how much opioid pain management they need. However, this information is relative and the contents and doses of drugs are highly variable.
- Many patients will experience anxiety related to undertreated pain. It is vital to treat patients in a caring and supportive manner and regularly reassess their pain. Communicate with the patient and use shared decision making to create a plan if their pain is not well controlled.
Pharmacotherapy
- Patients taking opioid agonist medications for OUD should continue their regular dose throughout their stay to improve outcomes.
- Treating pain often requires a multimodal approach. Additional pharmacological and non-pharmacological pain management should be explored. Adjunctive medications such as NSAIDs, acetaminophen, hydroxyzine, or clonidine may also reduce the dose of opioid needed to control pain.
- Methadone
- As a full agonist, methadone provides baseline OUD symptom control and does not block receptors.
- Short-acting opioids will bind freely and should be titrated to overcome tolerance for adequate pain control.
- Buprenorphine
- As a partial agonist, buprenorphine partially blocks receptors. It also has high receptor affinity.
- Even at high buprenorphine doses, full agonists can displace it when given at high enough doses.
- Opioids for analgesia will need to be given at higher doses than normal to outcompete buprenorphine to occupy opioid receptors.
- Increasing the daily dose of buprenorphine and/or split dosing may better control pain than a once daily dose.
- Naltrexone
- This protocol does not cover the care of patients on naltrexone. Consider expert consultation.
Special Populations
- Pregnancy and postpartum
- This protocol can be used for pregnant and postpartum patients; however, these are not comprehensive strategies for pain management during pregnancy and may not be sufficient to manage pain during labor. A pain management plan should be created with the patient and other specialists as needed.
- Extra care should be taken to prevent opioid withdrawal in pregnancy. Severe withdrawal impacts placental function and increases the risk of stunted growth, preterm labor, fetal convulsions, and fetal death.
- Consider regional anesthesia for perioperative pain management in patients that undergo cesarean section.
- MOUD is safe and effective for pregnant and breastfeeding parents and their newborns and is recommended by the American College of Obstetricians and Gynecologists (ACOG).
- After delivery, newborns should be monitored for neonatal opioid withdrawal syndrome (NOWS) for 3-7 days while following the Eat, Sleep, Console method.
- Breastfeeding is encouraged while on MOUD. Newborns of patients receiving additional short-acting opioids for pain should be monitored for somnolence.
- Adolescents: consider expert consultation.
Discharge planning
- If the patient is discharged with a prescription opioid for pain, ensure they continue to take their methadone or buprenorphine and have a plan to discontinue the short-term opioid. Patients may need additional support with medication management during this time.
- Patients on methadone
- Patients continuing or starting methadone may be dispensed up to a 3-day supply of methadone at discharge to bridge the gap to follow up care with their opioid treatment program (OTP), in accordance with 21 CFR 1306.07(b).
- Schedule a follow-up appointment with the OTP. The appointment must occur within 3 days of discharge to avoid missing doses.
- Patients on buprenorphine
- Split dosing of buprenorphine can help manage pain. Discuss dividing their regular buprenorphine dose into 3 daily doses. Educate the patient on additional pain management options such as over-the-counter medications and non-pharmacological interventions.
- In Washington, emergency departments are required to dispense naloxone to patients with OUD or others who are at risk of opioid overdose in compliance with SB5195. Ensure patient is discharged with naloxone in hand.
- When possible, connect patients with supports such as social workers, care navigators, or peers to improve patient experience and strengthen linkage to care.
Discharge Instructions
- Continue taking buprenorphine or methadone at your regular dose. It is okay to take this medication along with the other medications you were prescribed today.
- Tell your buprenorphine or methadone provider that you have a painful condition and what medications you were given today. It is common for people on medications for opioid use disorder to need additional medications when they have severe pain.
- Use other pain management strategies as well, including getting into a comfortable position, using heat, cold, and over-the-counter medications like acetaminophen and ibuprofen.
References
- American Psychiatric Association. Treatment of opioid use disorder in the general hospital. Approved by the Joint Reference Committee, October 2022. American Psychiatric Association; 2022:59. https://www.psychiatry.org/getattachment/879082d5-af6b-4c26-86e5-152bd53012b5/Resource-Document-Treatment-of-OUD-in-General-Hospital.pdf
- Crotty K, Freedman KI, Kampman KM. Executive summary of the focused update of the ASAM National Practice Guideline for the treatment of opioid use disorder. J Addict Med. 2020;14(2):99-112. doi:10.1097/ADM.0000000000000635
- De Aquino JP, Parida S, Avila-Quintero VJ, et al. Opioid-induced analgesia among persons with opioid use disorder receiving methadone or buprenorphine: A systematic review of experimental pain studies. Drug Alcohol Depend. 2021;228:109097. doi:10.1016/j.drugalcdep.2021.109097
- Englander H, Thakrar AP, Bagley SM, Rolley T, Dong K, Hyshka E. Caring for hospitalized adults with opioid use disorder in the era of fentanyl: a review. JAMA Intern Med. 2024;184(6):691-701. doi:10.1001/jamainternmed.2023.7282
- Kampman K, Jarvis M. American Society of Addiction Medicine (ASAM) National Practice Guideline for the Use of Medications in the Treatment of Addiction Involving Opioid Use. J Addict Med. 2015;9(5):358-367. doi:10.1097/ADM.0000000000000166
- Merlin JS, Khodyakov D, Arnold R, et al. Expert Panel Consensus on Management of Advanced Cancer-Related Pain in Individuals With Opioid Use Disorder. JAMA Netw Open. 2021;4(12):e2139968. Published 2021 Dec 1. doi:10.1001/jamanetworkopen.2021.39968
- Thakrar AP, Lowenstein M, Greysen SR, Delgado MK. Trends in Before Medically Advised Discharges for Patients With Opioid Use Disorder, 2016-2020. JAMA. 2023;330(23):2302-2304. doi:10.1001/jama.2023.21288
- Veazie S, Mackey K, Peterson K, Bourne D. Managing Acute Pain in Patients Taking Medication for Opioid Use Disorder: a Rapid Review. J Gen Intern Med. 2020;35(Suppl 3):945-953. doi:10.1007/s11606-020-06256-5

