
Considerations
Consider differential diagnoses, including non-accidental trauma, subdural hemorrhage, alcoholic ketoacidosis, sepsis, delirium, other acute intoxication or withdrawal, and hypo- or hyper-glycemia.
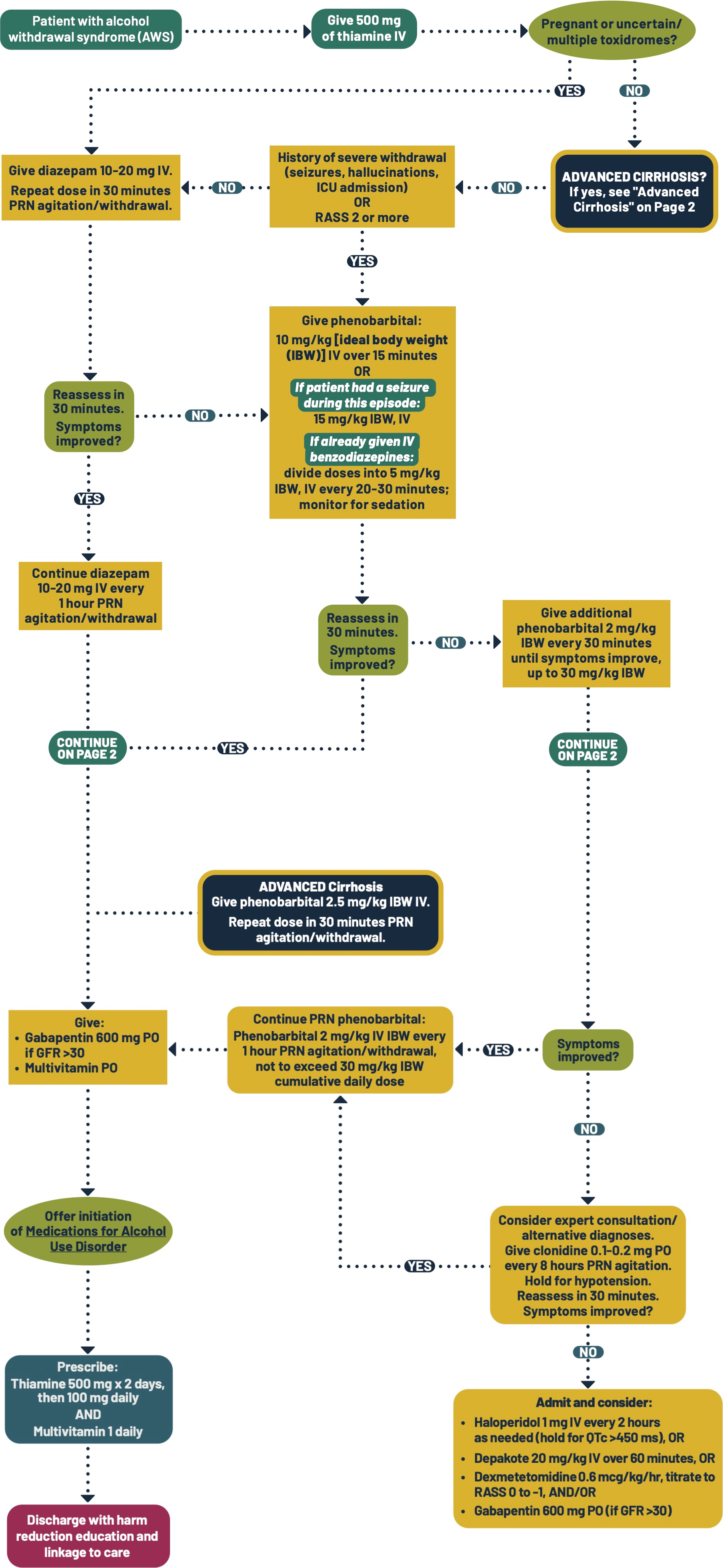
Assess for Wernicke's encephalopathy, which is an underdiagnosed neurologic emergency; early treatment with 500 mg thiamine IV is critical.
Consider admission for patients with a history of complicated alcohol withdrawal syndrome (AWS).
Do not use phenobarbital and consider expert consultation in patients who:
- Are pregnant
- Have uncertain or multiple toxidromes (e.g., concurrent opioid and/or benzodiazepine withdrawal, stimulant intoxication, etc.)
Phenobarbital doses are calculated by Ideal Body Weight (IDW), not actual weight. Max dose of 30mg/kg/day is recommended.
IV administration of diazepam and phenobarbital is recommended to better titrate and assess effect. Thiamine should also be given IV for rapid and improved absorption.
The RASS score is used in this protocol instead of CIWA because it is simple, quick, and performs just as well as CIWA in the setting of alcohol withdrawal.
Additional Clinical Guidance
- Alcohol use disorder (AUD) is treatable.
- Pharmacotherapy is evidence-based.
- Recovery often requires multiple treatment attempts.
- Stigma prevents help-seeking and worsens health outcomes.
- Care teams must challenge biases to provide compassionate, evidence-based care.
- Use non-stigmatizing, person-first language and trauma-informed care to promote engagement
Assessment
- The Richmond Agitation-Sedation Scale (RASS) is used to assess level of agitation, alertness, and sedation. The scale ranges from +4 (very agitated) to -5 (very sedated), with 0 representing an alert and calm state. Therapeutic goal is RASS 0 to –1.
- Advantages of RASS over CIWA-Ar for assessing alcohol withdrawal:
- RASS is a rapid, single-item scale that does not require patients to answer questions.
- CIWA-Ar can only be used in awake and alert patients and takes longer to assess.
- CIWA-Ar may be used in addition or as an alternative
Labs
- Phenobarbital has predictable, linear pharmacokinetics; thus, serum levels generally do not need to be checked when remaining within the recommended dose of no more than 20mg/kg/day. Seek expert consultation if you consider exceeding this dose. Toxicity occurs with plasma levels >40 mcg/mL.
Pharmacotherapy
- Phenobarbital is increasingly recommended over benzodiazepines to treat AWS; it is
preferred because:- Studies comparing phenobarbital and benzodiazepine monotherapy have shown fewer ICU admissions from the ED and shorter hospital stays with fewer adverse events (physical restraints, intubation) after admission in those given phenobarbital over benzodiazepines.
- Patients who receive phenobarbital are significantly less likely to return to the ED within 72 hours and have not been shown to experience more adverse events.
- Phenobarbital affects both inhibitory (GABA) and excitatory (glutamate) neurotransmitters. Benzodiazepines potentiate the GABA receptor, which helps calm the patient, but have no effect on excitatory neurotransmitters, which can cause paradoxical agitation.
- Phenobarbital has a rapid onset (5-20 min) and loading doses have a predictable, linear relationship to serum levels, and its maximum sedating effect occurs within 15 minutes of IV administration. It also has a long half-life (approximately 100 hours) with active metabolites, self-titrating over 3-4 days. This means that clinicians will see the deepest sedation while the patient is in the emergency department, but the protection from withdrawal symptoms will last for days after discharge.
- Benzodiazepines may cause delirium and be misinterpreted as ongoing
alcohol withdrawal.
- Diazepam (Valium) is preferred over chlordiazepoxide (Librium) in acute care
settings because:- Diazepam can be given orally or IV with peak sedation within 30-45 minutes.
- Use of chlordiazepoxide results in unpredictable levels of sedation due to delayed peak effect.
- Diazepam has a longer half-life (30-56 hour) with active metabolites, so therapeutic effect is extended.
- Patients who receive chlordiazepoxide often need a prescription to dose after discharge due to its shorter half-life (24-48 hours) and lack of active metabolites. After discharge, patients are at risk of oversedation if they combine chlordiazepoxide with alcohol.
- Multiple or uncertain toxidrome(s):
- Benzodiazepines are the best first-line therapy when the diagnosis is unclear or multiple toxidromes (e.g., concurrent opioid and/or benzodiazepine withdrawal, stimulant intoxication, etc.) are present.
Pathophysiology
- Alcohol withdrawal syndrome (AWS) typically occurs within 1-3 days following abrupt cessation or considerable decrease in heavy, chronic alcohol use. AWS ranges from mild to severe and can be life threatening.
- AWS symptoms may include:
- Autonomic: tachycardia, tachypnea, dilated pupils, elevated blood pressure, elevated body temperature, diaphoresis, nausea/vomiting, diarrhea.
- Motor: tremor, seizures, ataxia, gait disturbances, hyperreflexia, dysarthria.
- Psychiatric: irritability, anxiety, agitation, insomnia, delirium, disorientation, illusions, delusions, hallucinations, affect instability, disinhibition.
- Vitamin deficiency:
- Patients are at high risk for thiamine (vitamin B1) and folate deficiency and should receive supplementation.
- Thiamine supplementation prevents and treats Wernicke encephalopathy, which is life threatening.
- Electrolyte imbalance:
- Hyponatremia is common, especially amongst those who drink beer. This can be repleted with isotonic fluids.
- Hypokalemia is common and should be corrected.
- Patients are at risk for hypokalemia, hypophosphatemia and refeeding syndrome, and metabolic acidosis/alcohol-related ketoacidosis.
- Severe/complicated AWS:
- Severe AWS refers to seizures, autonomic dysfunction, delirium, and Wernicke encephalopathy.
- Risk factors for severe withdrawal include history of severe AWS, medical comorbidities, and co-dependence on benzodiazepines.
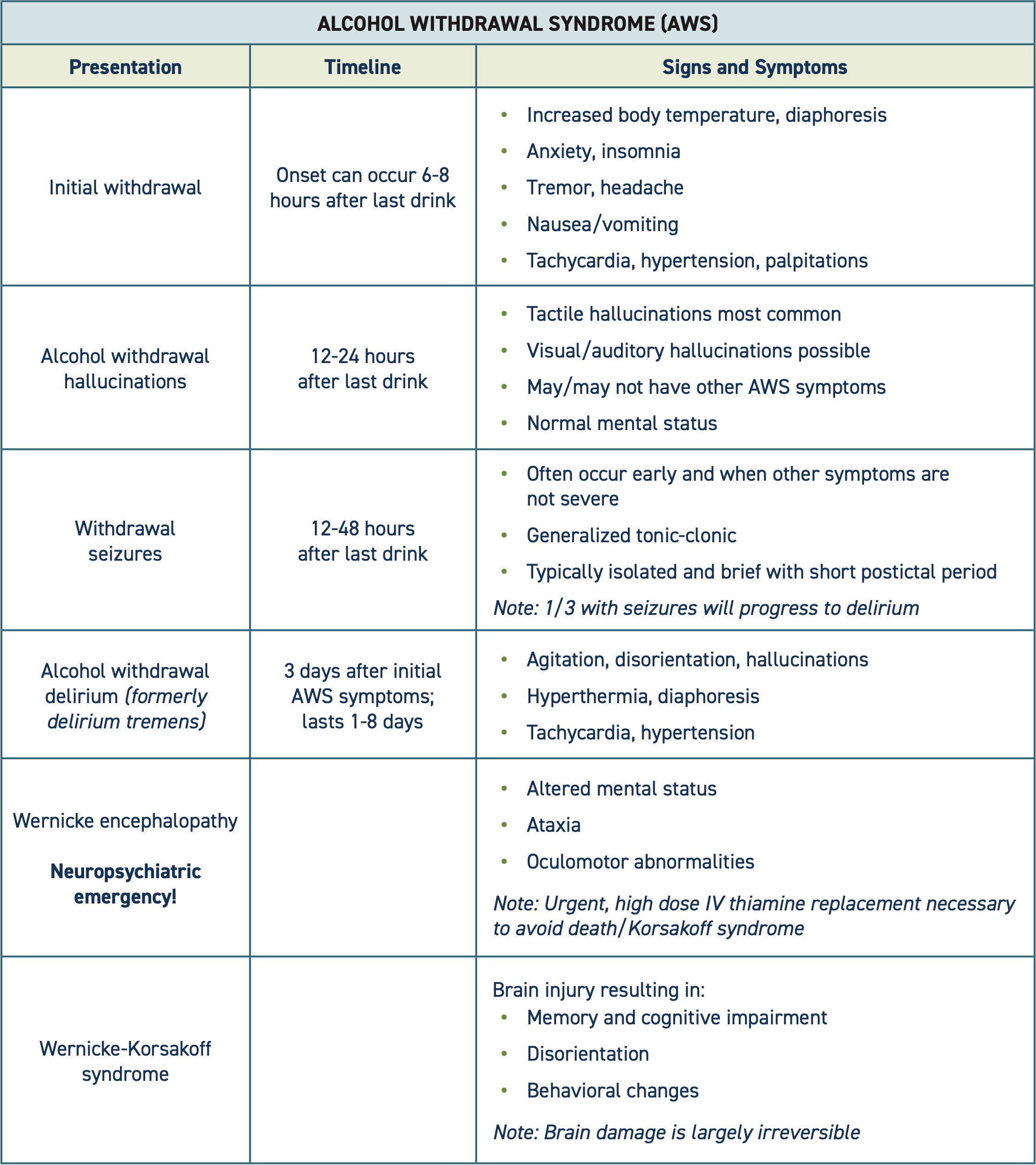
Table adapted from Gottlieb et al. (2024) and Canver et al. (2024).
Special populations
- Phenobarbital is contraindicated in pregnancy.
Patient safety
- Monitor and maintain adequate fluid intake and electrolyte balance. Ensure thiamine and folate supplementation for all AWS patients.
- If a patient is at risk for or experiencing severe AWS, administer indicated medications immediately to prevent complications.
- Patients with symptoms of Wernicke’s encephalopathy must be urgently treated with IV thiamine.
Discharge planning
- Arrange transfer to withdrawal management facility for ongoing management, if
indicated/preferred by patient. - Help the patient schedule a follow up appointment with primary care.
- Ask the patient if they have an established provider and where they want to receive ongoing care.
- Assist the patient with scheduling appointments and addressing barriers, like transportation. Refer to social work, if available.
- Outpatient and inpatient/residential treatment programs can be found on the Department of Health’s Behavioral Health Agency Greenbook.
- Discharge medications for AWS:
- Most patients who receive diazepam or phenobarbital will not require a prescription for medications to treat ongoing AWS symptoms after discharge.
- If the patient feels they need medications after discharge, consider gabapentin (first-line) or chlordiazepoxide (second-line):
- Gabapentin 600mg TID
- Gabapentin is preferred over a benzodiazepine due to less sedation risk.
- Patient should have normal GFR and be under 65 years old.
- Patient may continue this medication long term for management of AUD. See Medications for Alcohol Use Disorder.
- If patient chooses not to continue gabapentin long term, advise against abrupt discontinuation due to seizure risk. Consider the following taper:
- Gabapentin 300 mg tabs
- Day 1: 1 tab every 6 hours
- Day 2: 1 tab every 8 hours
- Day 3: 1 tab every 12 hours
- Day 4: 1 tab
- May have one additional tab every 12 hours as needed x 5
- Dispense #15
- Chlordiazepoxide
- Note delayed peak sedation and risk of oversedation if combined with alcohol. Discuss the risks and explain that the medication must not be combined with alcohol or other sedating substances.
- Chlordiazepoxide is preferred over diazepam when unobserved because it is less sedating.
- Prescribe:
- Day 1: 50mg every 6 hours
- Day 2: 25mg every 6 hours
- Day 3: 25mg every 12 hours
- Day 4: 25mg at night
- Dispense #15, no refills
- Do not use if consuming alcohol or taking other sedatives
- Gabapentin 600mg TID
- Offer medications to treat alcohol use disorder. See Medications for Alcohol Use Disorder.
- Provide naloxone for patients that use any street drugs and discuss safer use
strategies, including not using alone
Patient education
Educate patients on:
- Strategies to reduce the harms of alcohol (see Discharge Instructions).
- Treatment options for alcohol use disorder (see Related Protocols).
- The risks of combining alcohol with sedating substances.
Discharge Instructions
Treatment services
- Medications for alcohol use disorder can help you reduce or stop drinking and feel better. Talk to your health care provider about options.
- Contact the Washington Recovery Help Line at 866-789-1511 to learn about substance use treatment options.
- Peer support, like AA or Smart Recovery, may be helpful. Ask your care team about available local and online resources.
Reduce the harms of drinking
If you continue drinking, follow these tips to reduce some of the harms alcohol can cause:
- Don’t drink and drive. Have a safe transportation plan before you start drinking.
- Eat and drink water before you drink alcohol.
- Drink tea, water or other non-alcoholic beverages between drinks.
- Space out the time between drinks.
- Buy/order smaller servings.
- Drink beer or other lower alcohol content drinks instead of liquor.
- Drink slowly and take sips.
- Avoid drinking rounds, especially with friends who drink heavily.
- Avoid topping up your drink before it is empty.
- Limit the amount of alcohol you keep in your home.
- Schedule drinking and non-drinking days.
- Avoid mixing alcohol with other drugs or medications that make you sleepy. The combination could make you so sleepy that you stop breathing. If you do use drugs with alcohol, try not to use alone, so that someone can call 911 if you stop breathing.
CAUTION
- During your visit, you may have received medications that make you sleepy. Avoid alcohol and other medications or drugs that can make this worse. The combination could make you so sleepy that you stop breathing. Do not drive until these medications wear off.
- Know the signs and symptoms of alcohol poisoning: vomiting, loss of consciousness, decreased breathing, confusion, seizures, clammy skin. This is a medical emergency.
- If you are dependent on alcohol, do not stop drinking suddenly. Stopping suddenly can cause withdrawal that may be dangerous. Work with a medical provider to get medications to help you withdrawal from alcohol safely.
References
- Alwakeel M, Alayan D, Saleem T, et al. Phenobarbital-Based Protocol for Alcohol Withdrawal Syndrome in a Medical ICU: Pre-Post Implementation Study. Crit Care Explor. 2023;5(4):e0898. Published 2023 Apr 18.
doi:10.1097/CCE.0000000000000898 - Ammar MA, Ammar AA, Rosen J, Kassab HS, Becher RD. Phenobarbital Monotherapy for the Management of Alcohol Withdrawal Syndrome in Surgical-Trauma Patients. Ann Pharmacother. 2021;55(3):294-302.
doi:10.1177/1060028020949137 - Anton RF, Myrick H, Wright TM, Latham PK, Baros AM, Waid LR, Randall PK. Gabapentin combined with naltrexone for the treatment of alcohol dependence. Am J Psychiatry. 2011;168(7):709-717. doi:10.1176/appi.ajp.2011.10101436
- ASAM Clinical Practice Guideline on Alcohol Withdrawal Management. Journal of Addiction Medicine 14(3S):p 1-72, May/June 2020. | DOI:10.1097/ADM.0000000000000668
- Azim W, Walker R. Wernicke's encephalopathy: a frequently missed problem. Hosp Med. 2003;64(6):326-327. doi:10.12968/hosp.2003.64.6.326
- Backus TC, Hoffman RS. A Response to Nejad S et al.: Phenobarbital for Acute Alcohol Withdrawal Management in Surgical Trauma Patients-A Retrospective Comparison Study. Psychosomatics. 2020;61(6):855. doi:10.1016/j.psym.2020.05.020
- Borgundvaag B, Bellolio F, Miles I, et al. Guidelines for Reasonable and Appropriate Care in the Emergency Department (GRACE-4): Alcohol use disorder and cannabinoid hyperemesis syndrome management in the emergency department. Acad Emerg Med. 2024;31(5):425-455. doi:10.1111/acem.14911\
- Bosch NA, Crable EL, Ackerbauer KA, et al. Implementation of a Phenobarbital-based Pathway for Severe Alcohol Withdrawal: A Mixed-Method Study. Ann Am Thorac Soc. 2021;18(10):1708-1716. doi:10.1513/AnnalsATS.202102-121OC
- Canver BR, Newman RK, Gomez AE. Alcohol Withdrawal Syndrome. [Updated 2024 Feb 14]. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2025 Jan-. Available from: https://www.ncbi.nlm.nih.gov/books/NBK441882/
- Collins SE, Clifasefi SL. Safer Use Strategies: Alcohol. 2023. https://depts.washington.edu/harrtlab/wordpress/wp-content/uploads/2023/10/Safer-Use-Strategies-Alcohol-8.17.23.jpg
- Farkas J. Pulmcrit- Evidence Update: Phenobarbital in Alcohol Withdrawal.EmCrit.org. Published July 15, 2019. Accessed [date]. https://emcrit.org/pulmcrit/phenobarb-sampler/
- Gottlieb M, Chien N, Long B. Managing Alcohol Withdrawal Syndrome. Ann Emerg Med. 2024;84(1):29-39. doi:10.1016/j.annemergmed.2024.02.016
- Hammond CJ, Niciu MJ, Drew S, Arias AJ. Anticonvulsants for the treatment of alcohol withdrawal syndrome and alcohol use disorders. CNS Drugs. 2015;29(4):293-311. doi:10.1007/s40263-015-0240-4
- Hammond DA, Rowe JM, Wong A, Wiley TL, Lee KC, Kane-Gill SL. Patient Outcomes Associated With Phenobarbital Use With or Without Benzodiazepines for Alcohol Withdrawal Syndrome: A Systematic Review. Hosp Pharm. 2017;52(9):607-616.
- Hendey GW, Dery RA, Barnes RL, Snowden B, Mentler P. A prospective, randomized, trial of phenobarbital versus benzodiazepines for acute alcohol withdrawal. Am J Emerg Med. 2011;29(4):382-385. doi:10.1016/j.ajem.2009.10.010
- Ibarra F Jr. Single dose phenobar bital in addition to symptom-triggered lorazepam inalcohol withdrawal. Am J Emerg Med. 2020;38(2):178-181. doi:10.1016/j.ajem.2019.01.053
- Jesse S, Bråthen G, Ferrara M, et al. Alcohol withdrawal syndrome: mechanisms, manifestations, and management. Acta Neurol Scand. 2017;135(1):4-16. doi:10.1111/ane.12671
- Kessel KM, Olson LM, Kruse DA, Lyden ER, Whiston KE, Blodgett MM, Balasanova AA. Phenobarbital Versus Benzodiazepines for the Treatment of Severe Alcohol Withdrawal. Ann Pharmacother. 2024;58(9):877-885.
- Latt N, Dore G. Thiamine in the treatment of Wernicke encephalopathy in patients with alcohol use disorders. Intern Med J. 2014;44(9):911-915. doi:10.1111/imj.12522
- Lebin JA, Mudan A, Murphy CE 4th, Wang RC, Smollin CG. Return Encounters in Emergency Department Patients Treated with Phenobarbital Versus Benzodiazepines for Alcohol Withdrawal. J Med Toxicol. 2022;18(1):4-10. doi:10.1007/s13181-021-00863-2
- Malone D, Costin BN, MacElroy D, Al-Hegelan M, Thompson J, Bronshteyn Y. Phenobarbital versus benzodiazepines in alcohol withdrawal syndrome. Neuropsychopharmacol Rep. 2023;43(4):532-541. doi:10.1002/npr2.12347
- Mason BJ, Quello S, Goodell V, Shadan F, Kyle M, Begovic A. Gabapentin treatment for alcohol dependence: a randomized clinical trial. JAMA Intern Med. 2014;174(1):70-77. doi:10.1001/jamainternmed.2013.11950
- Nelson AC, Kehoe J, Sankoff J, Mintzer D, Taub J, Kaucher KA. Benzodiazepines vs barbiturates for alcohol withdrawal: Analysis of 3 different treatment protocols. Am J Emerg Med. 2019;37(4):733-736. doi:10.1016/j.ajem.2019.01.002
- Nisavic M, Nejad SH, Isenberg BM, et al. Use of Phenobarbital in Alcohol Withdrawal Management - A Retrospective Comparison Study of Phenobarbital and Benzodiazepines for Acute Alcohol Withdrawal Management in General Medical Patients. Psychosomatics. 2019;60(5):458-467. doi:10.1016/j.psym.2019.02.002
- Oks M, Cleven KL, Healy L, et al. The Safety and Utility of Phenobarbital Use for the Treatment of Severe Alcohol Withdrawal Syndrome in the Medical Intensive Care Unit. J Intensive Care Med. 2020;35(9):844-850. doi:10.1177/0885066618783947
- Patel S, Topiwala K, Hudson L. Wernicke's Encephalopathy. Cureus. 2018;10(8):e3187. doi:10.7759/cureus.3187
- Rosenson J, Clements C, Simon B, et al. Phenobarbital for acute alcohol withdrawal: a prospective randomized double-blind placebo-controlled study. J Emerg Med. 2013;44(3):592-598.e2. doi:10.1016/j.jemermed.2012.07.056
- Shah P, Stegner K, Rachid M, Hanif T, Dodd KW. Front-loaded Phenobarbital Dosing Is Associated with a Lower Incidence of Mechanical Ventilation in Patients with Severe Alcohol Withdrawal. Am J Respir Crit Care Med. 2019;199:A4144. doi:10.1164/ajrccm-conference.2019.199.1_meetingabstracts.a4144
- Sullivan SM, Dewey BN, Jarrell DH, Vadiei N, Patanwala AE. Comparison of phenobarbital-adjunct versus benzodiazepine-only approach for alcohol withdrawal syndrome in the ED. Am J Emerg Med. 2019;37(7):1313-1316. doi:10.1016/j.ajem.2018.10.007
- Tidwell WP, Thomas TL, Pouliot JD, Canonico AE, Webber AJ. Treatment of Alcohol Withdrawal Syndrome: Phenobarbital vs CIWA-Ar Protocol. Am J Crit Care. 2018;27(6):454-460. doi:10.4037/ajcc2018745
- Umar Z, Rasool MH ul, Muhammad S, et al. Phenobarbital and Alcohol Withdrawal Syndrome: A Systematic Review and Meta-Analysis. Cureus. 2023;15(1):e33695.

