
Considerations
Potential complicating factors:
- Concurrent opioid use disorder
- Impaired renal function
- Liver failure
See full protocol for guidance on medication selection.
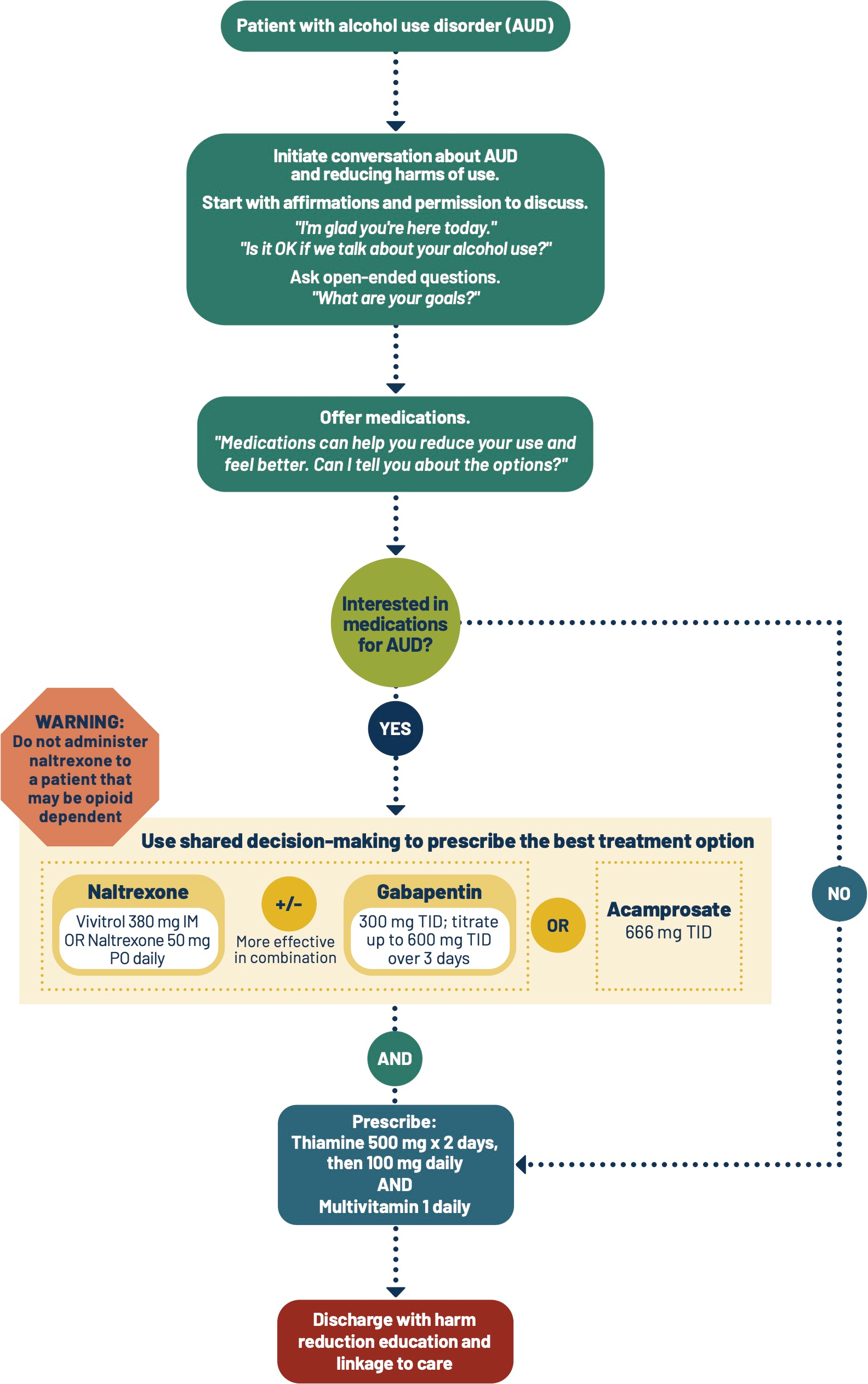
Naltrexone may precipitate delayed, long-lasting, and severe withdrawal symptoms in an opioid-dependent patient. Ask about opioid use and provide education prior to administration.
Patient Handouts
Additional Clinical Guidance
- Alcohol use disorder (AUD) is a treatable health condition. Recovery often requires multiple treatment attempts.
- AUD is highly prevalent and undertreated, with less than 2% of patients receiving evidence-based medications. An ED encounter is a valuable opportunity for intervention.
- Patients with AUD are stigmatized. Stigma prevents people from seeking care and worsens health outcomes. Providers should challenge biases to provide compassionate, evidence-based care.
Assessment
- Assess for opioid dependence and opioid use disorder (OUD) prior to initiating naltrexone.
- Consider screening for mental health comorbidities and referring to psychiatry as appropriate.
Pharmacotherapy
Use the following table and additional information below to aid in decision-making.
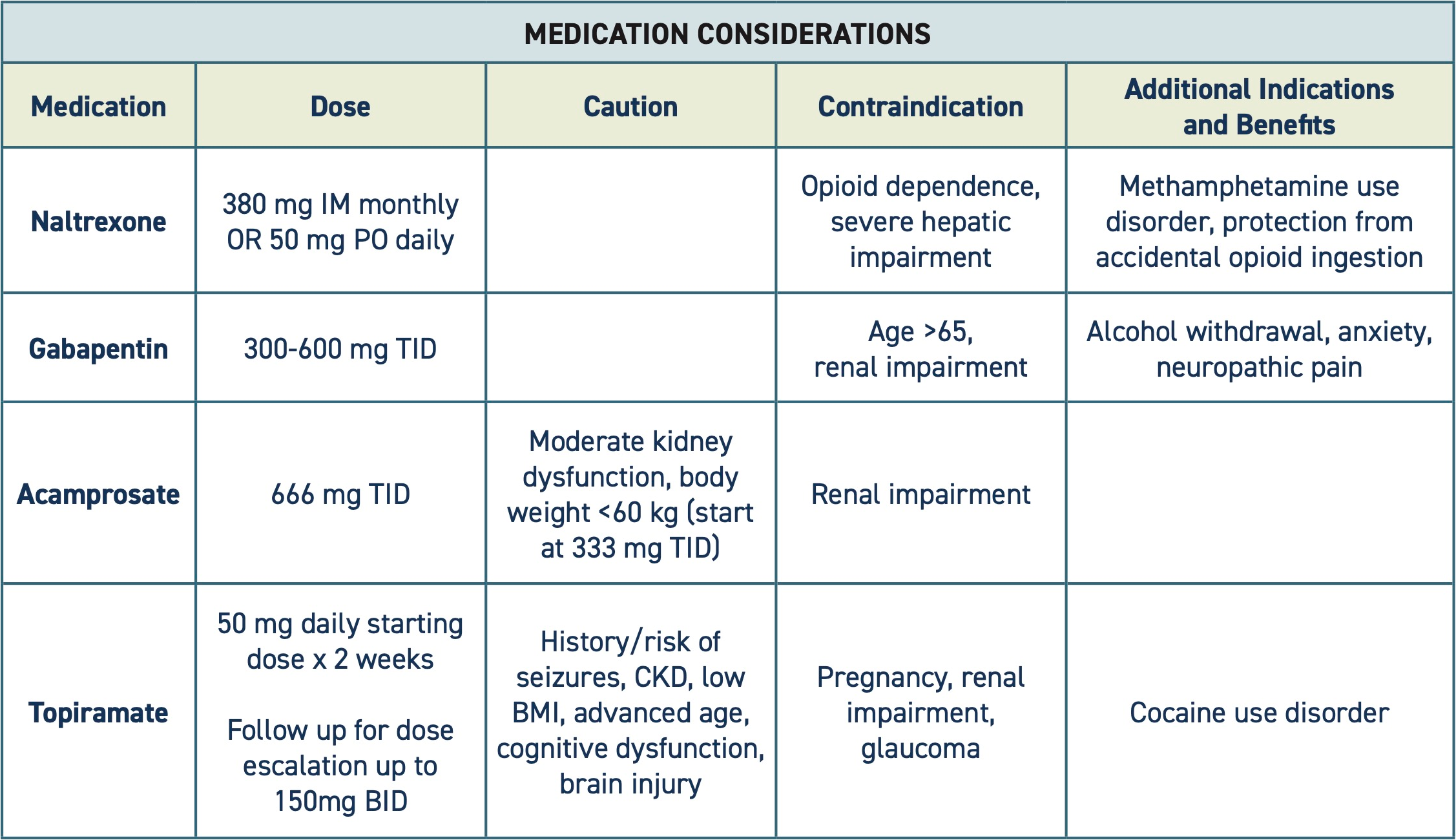
- Naltrexone
- Do not administer naltrexone to an opioid-dependent patient. Naltrexone is an opioid antagonist that can precipitate delayed, long-lasting, and severe withdrawal symptoms in an opioid-dependent patient.
- If dependency status is uncertain, consider a test dose of naloxone 0.4 mg, as it is shorter acting. Reassure the patient that if withdrawal occurs, symptoms will be treated. See Precipitated Withdrawal.
- If the patient has co-occurring opioid use disorder (OUD):
- Buprenorphine and methadone are the preferred treatments and cannot be combined with naltrexone.
- Naltrexone is a second-line option for OUD. It may be suitable to treat co-occurring OUD and AUD in some patients, such as in cases of prolonged abstinence from opioids, and with careful education regarding high overdose risk at treatment cessation.
- Offer long-acting injectable naltrexone (Vivitrol) for improved treatment adherence.
- Do not administer naltrexone to an opioid-dependent patient. Naltrexone is an opioid antagonist that can precipitate delayed, long-lasting, and severe withdrawal symptoms in an opioid-dependent patient.
- Gabapentin
- One RCT demonstrated that individuals receiving both gabapentin and naltrexone had improved drinking outcomes and improved sleep over those who receive naltrexone alone.
- Acamprosate
- Metanalyses demonstrate that acamprosate is efficacious in maintaining abstinence in those recently withdrawn from alcohol.
- An initial lower dose of 333 mg three times daily is recommended for individuals with moderate kidney dysfunction or body weight <60 kg.
- Three times daily dosing may be more difficult for patients to adhere to, compared to once daily naltrexone.
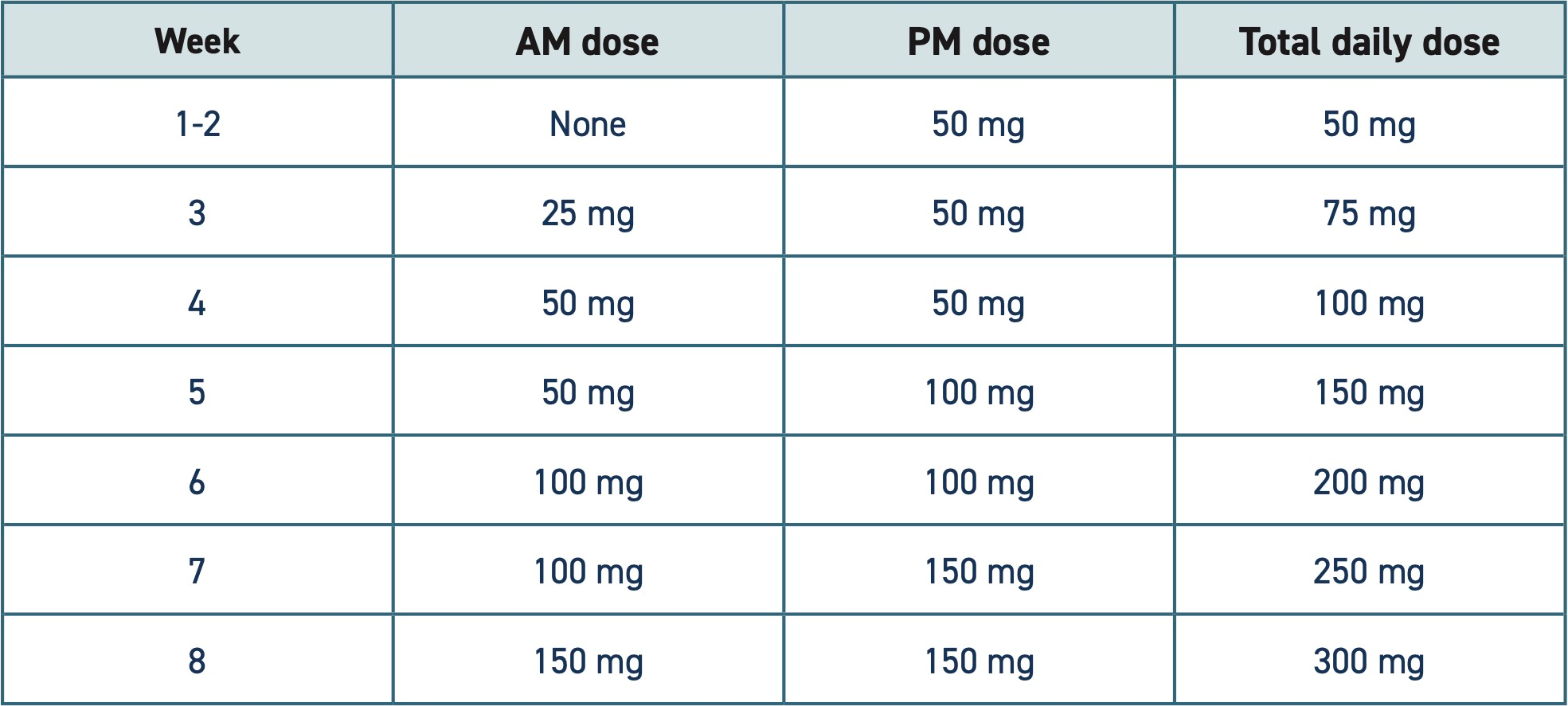
- Topiramate
- While appropriate for some patients, topiramate is not described in this protocol as a first-line option in the acute setting due to its side effect profile/lower tolerability, complexity of initiating/tapering, and incompatibility with several common medications, including warfarin, phenytoin, and divalproex, and the availability of other treatment options.
- Topiramate has been shown to decrease the number of heavy drinking days and has similar efficacy to naltrexone and acamprosate.
- Topiramate may be useful for patients with seizure disorders, with careful education on the risk of increased seizures with abrupt cessation.
- Topiramate may be a useful alternative for AUD treatment in those who do not tolerate or are poor candidates for other AUD medications.
- If topiramate is indicated, the following is a suggested dose escalation schedule:
Special populations
- Topiramate is contraindicated in pregnancy.
Polysubstance use
- Ask about other substance use and treat co-occurring substance use disorders as appropriate.
Patient safety
- Monitor for signs of Alcohol Withdrawal Syndrome (see Related Protocols).
- Patients with AUD are commonly deficient in thiamine and folate and should receive supplementation. Thiamine supplementation can prevent Wernicke encephalopathy, which is life threatening.
Discharge planning
- Help the patient schedule a follow up appointment with primary care.
- Ask the patient if they have an established provider and where they want to receive ongoing care.
- Assist the patient with scheduling appointments and addressing barriers, like transportation. Refer to social work, if available.
- Outpatient and inpatient/residential treatment programs can be found on the Department of Health’s Behavioral Health Agency Greenbook.
- Ensure patients are prescribed enough medication to last until their follow up appointment—at least 7-14 days is advised.
- Provide naloxone for patients that use any street drugs and discuss safer use strategies, including not using alone. Discharge medications for AWS.
Patient education
Educate patients on:
- Strategies to reduce the harms of alcohol (see Discharge Instructions).
- Treatment options for alcohol use disorder (see Related Protocols).
- The risks of combining alcohol with sedating substances.
Discharge Instructions
Medication Information
You may have been prescribed one or more of the following medications to help you reduce or stop your alcohol use. It is very important to continue taking your prescribed medications until you follow up with your primary care provider.
- Naltrexone
- Side effects of naltrexone are often mild or temporary and may be reduced with lower doses. Headache, nausea, and trouble sleeping are most common, and these typically go away over time.
- Do not take this medication if you are actively using opioid medications or drugs such as fentanyl, oxycodone, heroin, buprenorphine, or methadone. Naltrexone blocks the effect of opioids and can cause withdrawal if you are dependent on opioids.
- Stop taking this medication and return to the emergency department if you have stomach pain lasting more than a few days, dark urine, or yellowing of the skin or whites of the eyes.
- Vivitrol (injectable naltrexone)
- This medication is a form of naltrexone (described above) that is given as a monthly injection instead of a daily pill.
- Acamprosate
- If you miss a dose of this medication, take it as soon as possible. Do not take double doses to catch up. Do not crush the medication.
- Side effects may include sadness, irritability, lack of appetite, sleeplessness, tiredness, and trouble concentrating.
- Contact your provider immediately if you experience severe depression, fear, and/or thoughts of self-harm (rare).
- Gabapentin
- Common side effects include mild sedation, drowsiness, and dizziness. If any of these symptoms become severe, please stop taking this medication and seek medical attention.
- Taking this medication while using opioids or other sedating medications can cause excessive drowsiness and may interfere with breathing. Do not take it if you are already drowsy from other medications.
Topiramate
- Topiramate needs to be started at a low dose and increased over time.
- Do not stop taking this medication abruptly. If you do, you could have a seizure.
- If you choose to stop the medication, it must be slowly tapered down. Talk with your health care provider to help with this.
- Do not take this medication if you are pregnant or may become pregnant.
- Topiramate can harm the fetus.
- Topiramate may decrease the effectiveness of hormonal contraception (birth control). Talk to your provider about what kind of birth control may be best while taking this medication.
- Do not take if you have kidney problems or glaucoma (high pressure in your eye).
- Common side effects include nausea/diarrhea, feeling sleepy, trouble thinking and remembering, dizziness, loss of appetite, and weight loss.
Supportive services
- Contact the Washington Recovery Help Line at 866-789-1511 for additional resources and support with substance use.
- Peer support, like AA or Smart Recovery, may be helpful for some people. Ask your health care team about what resources may be available in your community.
If you continue drinking, follow these tips to reduce some of the harms alcohol can cause:
- Don’t drink and drive. Have a safe transportation plan before you start drinking.
- Eat and drink water before you drink alcohol.
- Drink tea, water or other non-alcoholic beverages between drinks.
- Space out the time between drinks.
- Buy/order smaller servings.
- Drink beer or other lower alcohol content drinks instead of liquor.
- Drink slowly and take sips.
- Avoid drinking rounds, especially with friends who drink heavily.
- Avoid topping up your drink before it is empty.
- Limit the amount of alcohol you keep in your home.
- Schedule drinking and non-drinking days.
- Avoid mixing alcohol with other drugs or medications that make you sleepy. The combination could make you so sleepy that you stop breathing. If you do use drugs with alcohol, try not to use alone, so that someone can call 911 if you stop breathing.
CAUTION
- During your visit, you may have received medications that make you sleepy. Avoid alcohol and other medications or drugs that can make this worse. The combination could make you so sleepy that you stop breathing. Do not drive until these medications wear off.
- Know the signs and symptoms of alcohol poisoning: vomiting, loss of consciousness, decreased breathing, confusion, seizures, clammy skin. This is a medical emergency.
- If you are dependent on alcohol, do not stop drinking suddenly. Stopping suddenly can cause withdrawal that may be dangerous. Work with a medical provider to get medications to help you withdrawal from alcohol safely.
Additional Resources
References
- Anton RF, Myrick H, Wright TM, et al. Gabapentin combined with naltrexone for the treatment of alcohol dependence. Am J Psychiatry. 2011;168(7):709-717. doi:10.1176/appi.ajp.2011.10101436
- Borgundvaag B, Bellolio F, Miles I, et al. Guidelines for Reasonable and Appropriate Care in the Emergency Department (GRACE-4): Alcohol use disorder and cannabinoid hyperemesis syndrome management in the emergency department.
- Collins SE, Clifasefi SL. Safer Use Strategies: Alcohol. 2023. https://depts.washington.edu/harrtlab/wordpress/wp-content/uploads/2023/10/Safer-Use-Strategies-Alcohol-8.17.23.jpg
- Hammond CJ, Niciu MJ, Drew S, Arias AJ. Anticonvulsants for the treatment of alcohol withdrawal syndrome and alcohol use disorders. CNS Drugs. 2015;29(4):293-311. doi:10.1007/s40263-015-0240-4
- Johnson BA. Addiction medicine: Science and practice. Springer; 2011.
- Latt N, Dore G. Thiamine in the treatment of Wernicke encephalopathy in patients with alcohol use disorders. Intern Med J. 2014;44(9):911-915. doi:10.1111/imj.12522
- Mason BJ, Quello S, Goodell V, Shadan F, Kyle M, Begovic A. Gabapentin treatment for alcohol dependence: a randomized clinical trial. JAMA Intern Med. 2014;174(1):70-77. doi:10.1001/jamainternmed.2013.11950
- Morley KC, Kranzler HR, Luquin N, et al. Topiramate Versus Naltrexone for Alcohol Use Disorder: A Genotype-Stratified Double-Blind Randomized Controlled Trial. Am J Psychiatry. 2024;181(5):403-411. doi:10.1176/appi.ajp.20230666
- Palpacuer C, Duprez R, Huneau A, et al. Pharmacologically controlled drinking in the treatment of alcohol dependence or alcohol use disorders: a systematic review with direct and network meta-analyses on nalmefene, naltrexone, acamprosate, baclofen and topiramate. Addiction. 2018;113(2):220-237. doi:10.1111/add.13974
- Substance Abuse and Mental Health Services Administration. Key substance use and mental health indicators in the United States: Results from the 2023 National Survey on Drug Use and Health. HHS Publication No. PEP24-07-021, NSDUH Series H-1. 2024. https://www.samhsa.gov/data/report/2023-nsduh-annual-national-report
- Wachman EM, Saia K, Bressler J, Werler M, Carter G, Jones HE. Case Series of Individuals Treated With Naltrexone During Pregnancy for Opioid and/or Alcohol Use Disorder. J Addict Med. 2024;18(3):288-292. doi:10.1097/ADM.0000000000001293

